ECT: A Clinical Reference
A practical working reference for clinicians — dosing schedules, lead placement, medication regimens, physics and calculations, mechanism, evidence, and the referral process for the Prisma Health Neuromodulation Program.
Overview
Modern ECT bears little resemblance to its early-20th-century origins. It is performed under general anesthesia with muscle relaxation, titrated to individual seizure threshold, delivered with brief or ultrabrief-pulse square-wave stimulation, and monitored continuously with EEG and EMG. Despite 85+ years of clinical use, it remains the most effective treatment available for severe or treatment-resistant depression.
This page is organized to serve as a day-to-day working reference. The first half covers the practical aspects of delivering ECT: schedule, placement, dosing, medications, procedure, physics, and calculations. The second half covers background and context: history, mechanism of action, efficacy evidence, cognitive side effects, and special populations. The page ends with referral information for the Prisma Health Neuromodulation Program.
ECT schedule
A standard ECT course is divided into three phases: index, continuation, and maintenance. The specific cadence is individualized based on response trajectory, side effect burden, and relapse risk.
Index course
Index ECT is typically given 3 times per week, conventionally Monday / Wednesday / Friday. An average index course runs 9–12 treatments, though this varies considerably. Some patients respond after 6 sessions; others may require 15 or more to reach maximal benefit. The clinical plateau (two or more consecutive treatments without additional gain) is a reasonable indicator to transition out of the index phase.
Some centers use twice-weekly index scheduling, which produces comparable end-point efficacy with somewhat reduced cognitive burden at the cost of slower time-to-response. The choice depends on urgency, patient tolerance, and logistics.
Continuation
The continuation phase follows the index course and lasts approximately 6 months. Its purpose is to prevent early relapse during the high-risk post-index window. A typical taper:
- Week 1 post-index: 1 treatment
- Weeks 2–4: every 1–2 weeks
- Months 2–3: every 2–3 weeks
- Months 4–6: every 3–4 weeks
Maintenance
Maintenance ECT refers to treatments delivered more than 6 months after the index course, aimed at preventing recurrence. Frequency is individualized: monthly is common, but intervals of 6–8 weeks are also well-tolerated for stable patients. Indications favoring long-term maintenance ECT:
- Multiple prior episodes with rapid relapse off ECT
- Intolerance or inadequate response to continuation pharmacotherapy
- History of psychotic depression (higher recurrence risk)
- Strong prior response to ECT relative to other modalities
Maintenance ECT and continuation pharmacotherapy are not mutually exclusive; many patients do best on a combined strategy, particularly during the first year after an index course.
Lead placement
The three commonly used electrode configurations are bitemporal (bilateral), right unilateral (RUL), and bifrontal. Each has a distinct efficacy-to-cognitive-side-effect profile.

Common ECT electrode placements: bilateral (bitemporal), right unilateral (RUL), and bifrontal.
Right unilateral (RUL)
Both electrodes on the non-dominant (right) side of the head. Typically paired with an ultrabrief pulse width (0.3–0.37 ms) for optimal cognitive preservation. Requires suprathreshold dosing — typically 5–6× seizure threshold — for adequate efficacy. A reasonable default starting placement for many patients, particularly where cognitive side effects would be especially problematic.
Bilateral (bitemporal)
One electrode over each temple. Most efficacious per treatment and fastest time-to-response, but highest cognitive burden. Appropriate first-line choice in urgent presentations — catatonia, severe neurovegetative illness, psychotic depression, life-threatening inanition, or acute suicidality — where speed of response is clinically decisive.
Bifrontal
Both electrodes over the frontal lobes. Comparable efficacy to bitemporal in most comparative studies, with somewhat reduced memory effects. A useful middle-ground when bilateral stimulation is indicated but cognitive burden of bitemporal is a concern.
How to choose
Many clinicians start with RUL ultrabrief pulse, escalating to bilateral (bifrontal or bitemporal) if response is inadequate after 6–8 treatments. Start bilateral in high-acuity presentations where delay to response carries meaningful risk. The Kolshus 2017 meta-analysis (Cochrane Review) found comparable efficacy between high-dose RUL and bitemporal, with RUL showing advantages in reorientation time and retrograde memory preservation.
Dosing
ECT dose is properly expressed as electrical charge (millicoulombs), a function of amplitude, frequency, pulse width, and duration. Higher doses produce more reliable seizures and may work faster — but at the cost of increased cognitive burden. Individualized titration balances these tradeoffs.
Why titrate?
Seizure threshold varies across patients by a factor of 40 or more. Fixed-dose approaches risk either under-dosing (subthreshold, inefficacious) or over-dosing (supratherapeutic, unnecessarily cognitively burdensome). Titration determines the individual seizure threshold at the first treatment, then dose subsequent treatments as a defined multiple of that threshold.
- Bitemporal / bifrontal: 1.5–2× seizure threshold is adequate for efficacy. Higher doses add cognitive burden without improving outcomes.
- Right unilateral: 5–6× seizure threshold is standard. Doses below 2.5× ST have minimal efficacy — this is the most common error in RUL ECT.
Dosing schedules
The dosing tables below reflect a standard titration approach used in clinical practice — originally developed and refined at the University of Michigan ECT program and broadly representative of current best practice.

Bilateral (bitemporal / bifrontal) titration schedule. Starting dose is determined empirically at the first treatment; subsequent treatments dose at approximately 1.5× seizure threshold.

Right unilateral titration schedule. Because RUL requires markedly suprathreshold dosing for efficacy, the titration curve is steeper and the maintenance dose is approximately 5–6× seizure threshold.
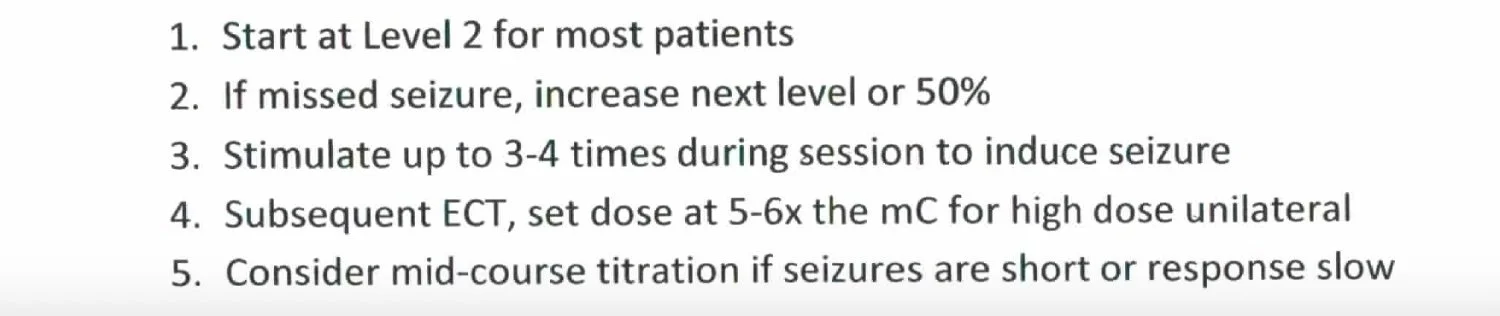
Practical notes and interpretation tips for the RUL titration schedule.
Seizure quality assessment
Duration alone is an incomplete measure of adequate ECT. Beyond the 25–60 second target window, seizure quality is assessed by:
- Ictal EEG morphology — high-amplitude polyspike activity, clear postictal suppression
- Postictal suppression index — higher isoelectric percentage post-ictally correlates with stronger seizure
- Heart rate response — adequate tachycardic response indicates adequate seizure generalization
- Midictal EEG amplitude — higher amplitudes correlate with greater clinical benefit
Adequate duration with poor quality (low amplitude, minimal postictal suppression, blunted HR response) warrants technical adjustment rather than simply continuing the course.
ECT medications
Most patients receive several medications at each ECT treatment, administered via IV. A typical regimen includes an anesthetic, a paralytic, an analgesic, an antiemetic, and an antimuscarinic. Doses are individualized to body mass, anesthetic response, and specific requirements.
Anesthetic
- Methohexital (Brevital) — 0.75–1 mg/kg. Traditional gold-standard ECT anesthetic. Short-acting with minimal elevation of seizure threshold.
- Etomidate — 0.2–0.3 mg/kg. Particularly useful in hemodynamically unstable patients; does not meaningfully raise seizure threshold. Post-ECT nausea somewhat more common than with methohexital.
Paralytic
- Succinylcholine — ~1 mg/kg. Standard choice for ECT; short-acting and compatible with brief procedure duration.
- Rocuronium — 0.5–1 mg/kg. Alternative when succinylcholine is contraindicated (e.g., pseudocholinesterase deficiency, malignant hyperthermia risk, hyperkalemia). Requires sugammadex reversal.
Analgesic
- Acetaminophen (Tylenol) — 500–1000 mg PO. Often given prophylactically for post-ECT headache.
- Ketorolac (Toradol) — 15–30 mg. For more pronounced post-ECT headache or myalgia.
Antiemetic
- Ondansetron (Zofran) — 4–8 mg
- Promethazine (Phenergan) — 6.25–12.5 mg
Additional agents (as clinically indicated)
- Glycopyrrolate — 0.1–0.4 mg. Bradycardia prevention and secretion control.
- Labetalol — 5–10 mg. Blunting of the hypertensive surge.
- Ketamine — 15–60 mg. Used selectively as anesthetic adjunct; may augment analgesia and lower seizure threshold.
- Flumazenil — 0.25–1 mg. Benzodiazepine reversal when BDZ burden is compromising seizure quality.
- Caffeine — 125–500 mg IV. Seizure augmentation in patients with difficult-to-elicit seizures.
- Midazolam (Versed) — 1–4 mg. Postictal agitation/anxiety or prolonged seizure termination.
- Sugammadex — weight-based. Rocuronium reversal.
The procedure itself
A typical ECT treatment visit runs 90–120 minutes door-to-door. The procedure itself — from anesthesia induction through wake-up — takes about 10–15 minutes.
- Arrival and check-in (15–20 min): NPO status confirmed, vital signs, brief clinical assessment covering interval symptom changes and any side effects from the prior session, informed consent reviewed.
- IV and monitoring setup (10–15 min): IV access, EKG, pulse oximetry, BP cuff, bilateral frontomastoid EEG electrodes, stimulation electrodes per planned placement, tourniquet on one limb for cuff-isolated motor seizure observation.
- Pre-oxygenation and induction (3–5 min): 100% O2 via mask, anesthetic administered IV, followed by paralytic. Bite block placed before stimulation.
- Stimulus delivery and seizure (1–2 min): Once the patient is adequately paralyzed and fasciculations have subsided, stimulus delivered. Seizure duration monitored on EEG and on the cuffed limb. Ideal seizure duration 25–60 seconds.
- Immediate recovery (5–10 min): Mask ventilation until spontaneous respiration resumes, then supplemental O2. Continuous vital sign monitoring.
- PACU-equivalent recovery (45–90 min): Extended observation until the patient is fully oriented, ambulating safely, tolerating PO, and meeting standard discharge criteria.
Common intra-procedure events and management
- Hypertensive surge: Expected and usually transient. Pre-treat with labetalol or esmolol in patients with cardiovascular disease or unusually large HR/BP responses.
- Bradycardia or asystole: Brief post-stimulation vagal response. Glycopyrrolate often given prophylactically, particularly for subthreshold stimulations and with propofol anesthesia.
- Prolonged seizure (>2 min): Terminate with midazolam or additional methohexital; ensure adequate ventilation throughout.
- Missed or inadequate seizure: Reassess anesthetic dose, consider hyperventilation before restimulation, check stimulus parameters and electrode contact; caffeine can be added for subsequent treatments if the pattern persists.
- Postictal agitation or confusion: More common in older patients. Ensure oxygenation, minimize sensory input, low-dose benzodiazepine if severe.
Physics of ECT
ECT dose is fundamentally a question of delivered electrical charge. Understanding the physics clarifies why modern parameter choices (square wave, brief/ultrabrief pulse, biphasic delivery) improve efficacy-to-side-effect ratios.
Video 1ECT physics explained — walkthrough of the core concepts.
Video 2ECT physics explained — continued.
Waveform
Early ECT devices delivered a sine wave — the natural waveform of alternating household current. This waveform is highly inefficient for neuronal depolarization: much of the delivered charge is "wasted" on subthreshold portions of the wave that don't contribute to depolarization but do contribute to cognitive side effects. Modern devices deliver a square wave, which is approximately equal in efficacy to sine-wave stimulation while requiring substantially less total charge.

Sine wave (top, older ECT devices) vs. square wave (bottom, modern ECT devices). Square-wave stimulation produces equivalent efficacy with substantially reduced charge and cognitive burden.
Most modern devices deliver a biphasic (bidirectional) square wave, effectively doubling the frequency — this must be accounted for in charge calculations.
Waveform parameters
Four parameters together determine the delivered dose:
- Amplitude (mA) — peak current, typically 800–900 mA in modern devices
- Frequency (Hz) — pulses per second (doubled for biphasic waveforms)
- Pulse width (ms) — duration of each individual pulse
- Train duration (s) — total duration of the stimulus

The four parameters that together determine delivered charge: amplitude, frequency, pulse width, and train duration.
Pulse width: brief vs. ultrabrief
Pulse width matters because neuronal chronaxie — the minimum time needed to produce depolarization at twice rheobase — is approximately 0.1–0.2 ms for cortical neurons (Peterchev 2010). Pulses longer than this are "wasted" charge from a depolarization standpoint.
- Brief pulse (0.5–1.5 ms): Standard modern waveform. Efficient relative to sine wave; produces adequate seizures with modest charge.
- Ultrabrief pulse (<0.5 ms, typically 0.25–0.37 ms): More closely matches cortical neuron chronaxie. Requires less total charge to produce seizures and is associated with significantly reduced cognitive side effects (Sackeim 2008). When paired with suprathreshold RUL stimulation, efficacy is preserved; with subtherapeutic RUL dosing, ultrabrief pulse can underperform.

Brief pulse vs. ultrabrief pulse. Ultrabrief pulse (<0.5 ms) more closely matches cortical neuron chronaxie and reduces cognitive burden when paired with adequate RUL dosing.
Calculations
The math behind ECT dosing, at a level sufficient for parameter adjustments and ballpark understanding of device settings.
Charge (dose)
ECT dose is measured in millicoulombs (mC). One coulomb equals approximately 6.24 × 1018 electrons. Since charge equals current times time:
0.8 × 0.00037 × 240 × 8 = 0.568 C
Energy delivered
Energy depends on the dynamic impedance during stimulation (typically 100–300 Ω in adequately prepped patients; static pre-stimulus impedance is much higher, 1000–2500 Ω):
0.82 × 220 × 0.7104 = 0.64 × 220 × 0.7104
Voltage
Voltage follows from energy and charge:
For most clinical purposes, the important number is charge in millicoulombs. Device interfaces express dose either as a percentage of maximum output, directly in mC, or as individual parameter settings. What's happening mechanically is the same: a specified amount of electrical charge, delivered over a specified duration, at a specified amplitude.
A brief history of ECT
Modern practice looks almost nothing like its origins. Knowing the history clarifies both the current technique decisions and the persistent stigma surrounding the treatment.
Meduna's pharmacologic convulsive therapy
Hungarian psychiatrist Ladislas Meduna, working on the (incorrect) hypothesis of a biological antagonism between epilepsy and schizophrenia, induces therapeutic seizures using camphor and later pentylenetetrazol (Metrazol). Patients often improve, but the pre-seizure experience is terrifying and the method is unreliable.
Cerletti and Bini — the first human ECT
Ugo Cerletti and Lucio Bini at Sapienza University of Rome, seeking a safer alternative to Metrazol, develop electrical seizure induction. Inspired partly by observing electrical stunning of pigs at a Roman slaughterhouse, they perform the first human ECT in April 1938, treating a patient with schizophrenia (identified in historical accounts as "Enrico X." and presenting with paranoid symptoms including delusions and hallucinations). The original technique used bitemporal sine-wave stimulation with no anesthesia and no muscle relaxation.
Rapid international adoption
ECT spreads globally within a few years. "Unmodified" ECT produces full tonic-clonic convulsions, and fracture of the spine and long bones is a recognized complication. Bennett's 1940 JAMA report describes early use of curare for muscle relaxation — an important precursor to modern modified ECT.
The modification era: anesthesia and succinylcholine
Introduction of short-acting barbiturate anesthesia (pentothal) and the paralytic succinylcholine transforms ECT from a visibly violent procedure into a modern anesthetic one. Muscle fractures disappear. Patients are unconscious and motionless during treatment. This is the "modified ECT" that remains the basis of modern practice.
The cultural backlash
Publication of Ken Kesey's One Flew Over the Cuckoo's Nest (1962) and the 1975 film adaptation cement a lasting public image of ECT as a punitive, dehumanizing procedure. Concurrent documented abuses in some institutions add credibility to the criticism. ECT use declines sharply in the US during this period.
The first major consensus statements
The NIH Consensus Conference on ECT (June 10–12, 1985; statement published in JAMA, October 18, 1985) and the APA Task Force Report (1978, revised 1990 and 2001) re-establish ECT as a valid, evidence-based treatment. These documents standardize technique, indications, consent, and training. Sackeim and colleagues' landmark studies begin clarifying the dose-response relationship between stimulus and both efficacy and cognitive effects.
Brief pulse, right unilateral, and titration
Wide adoption of brief-pulse square-wave stimulation (far more efficient than sine wave) and renewed interest in right-unilateral placement to reduce memory effects. Stimulus titration — individually determining seizure threshold — becomes standard.
Ultrabrief pulse and dose optimization
Introduction of ultrabrief pulse width (<0.5 ms) further reduces cognitive burden. Sackeim 2008 demonstrates that suprathreshold ultrabrief RUL preserves efficacy with markedly reduced cognitive side effects. Bifrontal placement gains popularity as a middle-ground bilateral approach.
FDA reclassification
After extensive review, the FDA reclassifies ECT devices from Class III (highest risk) to Class II for use in severe treatment-resistant or acutely life-threatening major depressive episodes associated with MDD or bipolar disorder, and for catatonia, in patients age 13 and above. Use for other indications (including mania, schizophrenia, and schizoaffective disorder) remains Class III. The reclassification legitimizes ECT's established indications while maintaining regulatory oversight.
Mechanism research, individualized dosing, and MST
Growing evidence on network-level mechanisms (subgenual cingulate, DMN), hippocampal neuroplasticity, and immunomodulatory effects. Magnetic seizure therapy (MST) has emerged as a viable alternative convulsive therapy. The confirmatory CREST-MST trial (Blumberger et al., Lancet Psychiatry 2026) showed MST non-inferior to RUL ultrabrief ECT for remission with a more favorable cognitive safety profile, supporting MST's consideration as an alternative convulsive therapy in MDD for patients concerned about ECT's cognitive effects. This complements earlier pilot data (Deng et al., JAMA Psychiatry 2024, n=73) showing comparable efficacy with faster time to reorientation. Precision approaches (amplitude titration, individualized E-field modeling) continue translating from research to clinical trials.
Mechanism of action
We understand ECT's clinical effects far better than its mechanisms. The field has converged on a multi-system model rather than any single pathway.
Monoamine system
Similar to pharmacologic antidepressants, ECT modulates synaptic serotonin, norepinephrine, and dopamine. Receptor sensitivity changes follow, leading to adaptive changes in the function of mood-relevant circuits. The monoamine framework alone, however, cannot explain ECT's speed or its efficacy in medication-refractory cases.
Neurotrophic factors
ECT upregulates BDNF in most studies (Brunoni 2014 meta-analysis) and has been reported to alter VEGF in smaller samples (Minelli 2011, n=19; replication remains inconsistent). Animal models show upregulation of c-Fos, Egr1, Neuritin 1, BDNF, SNAP-29, synaptotagmin III, synapsin I, and PSD-95 (Dyrvig 2014). The clinical correlation between BDNF changes and symptom improvement has not been consistently established, but the pattern of neurotrophic upregulation is reproducible.
HPA axis
Elevated cortisol is a common finding in severe depression. ECT appears to normalize HPA-axis dysregulation in many patients (Haskett 2014, review of neuroendocrine hypotheses). Whether this is a direct therapeutic mechanism or a downstream effect of clinical improvement remains debated.
Functional connectivity
Resting-state fMRI studies show ECT alters connectivity in depression-relevant networks. Beall 2012 demonstrated increased connectivity from the anterior cingulate cortex to the right dorsolateral prefrontal cortex and posterior cingulate cortex, with correlation to clinical improvement. More recent work (Perrin 2012; Mulders 2016; Sinha 2021 ALE meta-analysis) has focused on subgenual cingulate and default-mode network changes, with increasing convergence on DMN dysconnectivity as a candidate target.
GABA and glutamate
ECT has been associated with changes in GABAergic function (Esel 2008 measured serum GABA levels), potentially contributing to the anticonvulsant effects observed over the course. Cortical GABA changes have also been demonstrated using MR spectroscopy in separate studies. Glutamatergic modulation — acute increases in glutamate release followed by NMDA and AMPA receptor downregulation — is also well-described.
Neuroplasticity at the network level
Hippocampal volume increases after a course of ECT are a reliable MRI finding; the clinical significance remains debated. The volume change correlates with both antidepressant response and with cognitive side effects in different studies. Hippocampal enlargement may be a marker of a broader plasticity response rather than a specific therapeutic mechanism.
Evidence & outcomes
ECT has one of the largest evidence bases in psychiatry, including multiple RCTs against sham and head-to-head trials against pharmacotherapy and other neuromodulation.
ECT vs. sham ECT
The UK ECT Review Group (2003) summarized 6 RCTs (n=256) of real vs. sham ECT, with a pooled effect size of −0.91 (95% CI −1.27 to −0.54) in favor of real ECT. The review also concluded that ECT was significantly more effective than pharmacotherapy (18 trials, n=1144, SES −0.80).
Anderson 2021 reviewed 11 sham-controlled RCTs and 5 meta-analyses, concluding that "despite their methodological differences, there is a consistent direction in the findings of the RCTs of at least a numerical benefit for ECT over sham ECT... and all meta-analyses report a significant pooled result in favor of ECT."
Response and remission rates
| Population / Study | Response | Remission | Notes |
|---|---|---|---|
| Modern ECT overall (Belge 2024) | 70–80% | 50–60% | Even in treatment-resistant depression |
| CORE / Petrides 2001 (n=253) — psychotic | — | 95% | Psychotic features a strong positive predictor |
| CORE / Petrides 2001 — non-psychotic | — | 83% | 4-site bilateral ECT at 50% above threshold |
| CORE / Prudic 2007 (n=489) — melancholic | — | 62% | 311 of 489 had melancholic features |
| CORE / Prudic 2007 — non-melancholic | — | 79% | Melancholic features (counterintuitively) predicted lower remission |
| Keller 2025 (Pine Rest community clinic, n=35) | 54% | 31% | Lower than trials; baseline anxiety predicts poorer response |
| Royal College ECTAS (2023) | — | 41% | England/Wales/NI/Ireland national dataset; Scotland reported separately via SEAN |
| Ultrabrief RUL meta-analysis (Dunne 2025, n=1478) | — | 32% | Lower than brief-pulse; efficacy-cognitive tradeoff |
Parameter-specific comparative data
- Sackeim 1987 (n=52): Low-dose bilateral ECT (70% response) vs. low-dose RUL (28%). Early demonstration that RUL requires suprathreshold dosing.
- Sackeim 1993 (n=96): Threshold vs. 2.5×threshold, bilateral vs. RUL. Response rates: 2.5×ST bilateral 65%, threshold bilateral 63%, 2.5×ST RUL 43%, threshold RUL 17%.
- Sackeim 2000 (n=80): High-dose bilateral (150% above ST) and high-dose RUL (500% above ST) both 65% response; low-dose RUL substantially worse (30–35%).
- McCall 2000: Fixed-dose 403 mC RUL 67% response vs. 2.25×ST RUL 39%. Higher RUL doses produce better outcomes.
- Sackeim 2008: Ultrabrief RUL non-inferior to brief-pulse RUL for efficacy, with markedly reduced cognitive burden.
- Kolshus 2017 (meta-analysis): High-dose RUL comparable to bitemporal for efficacy; RUL superior for reorientation time and retrograde memory.
ECT vs. other treatments
Continuation treatment: the Sackeim 2001 CUC trial
Continuation treatment is not optional. Sackeim 2001 (the Columbia University Consortium trial) randomized 84 ECT-remitted patients to three continuation regimens:
- Placebo: 84%
- Nortriptyline monotherapy: 60%
- Nortriptyline + lithium: 39%
The CORE continuation trial (Kellner 2006) found continuation ECT non-inferior to combination pharmacotherapy for relapse prevention. For patients who cannot tolerate lithium or tricyclics, modern regimens substitute SSRIs/SNRIs + lithium or lamotrigine, with somewhat less robust supporting evidence.
Cognitive side effects
Cognitive effects are the most-discussed, most-feared, and most-important side effect of ECT. Their management is central to modern practice.
Domains of effect
- Acute postictal confusion: Universal; resolves spontaneously within minutes to hours.
- Anterograde memory impairment: Difficulty forming new memories during the course. Detectable on neuropsychological testing; typically resolves within weeks of course completion.
- Retrograde amnesia: Loss of memories from the period around treatment. Recent events are more affected than remote events (Ribot's law).
- Autobiographical memory gaps: The most persistent and patient-relevant effect. A minority of patients report long-lasting difficulty recalling specific life events from before or during treatment. Severity and duration are variable.
- Global cognitive slowing: Word-finding difficulty, reduced processing speed. Typically resolves within weeks to months.
The Semkovska 2010 meta-analysis
Semkovska and McLoughlin (2010) meta-analyzed cognitive outcomes across ECT studies, finding that most cognitive abnormalities are limited to the first 3 days post-treatment, and that pre-treatment functioning is subsequently recovered. Beyond day 15, processing speed, working memory, anterograde memory, and some aspects of executive function actually improve beyond baseline — almost certainly reflecting the lifting of depression-related cognitive impairment.
Technique choices that reduce cognitive burden
- RUL placement over bitemporal
- Ultrabrief pulse width over brief pulse (when paired with adequate suprathreshold dosing)
- Twice-weekly scheduling over thrice-weekly, when urgency permits
- Minimum effective stimulus dose rather than ceiling dosing
- Methohexital or etomidate over propofol when seizure threshold elevation is a concern
- Discontinuation of benzodiazepines and anticholinergics during the course when clinically feasible
A clinically useful framing
Patient subjective memory complaints after ECT often exceed objective deficits on neuropsychological testing. Both are real: the subjective experience is legitimate and warrants attention, and at the same time, severe depression itself causes significant cognitive impairment that typically improves with successful ECT. A candid framing at consent: "You'll likely have some memory disruption around the treatment period, and for most patients this resolves; a minority report longer-lasting gaps. We can choose placements and parameters to minimize these effects, at some tradeoff in speed of response."
Special populations
Older adults
ECT is more effective in older adults than younger adults, with higher remission rates and faster response. Older patients experience more cognitive side effects but these are typically transient, and medication side effects are often substantially more problematic than ECT in this population. For severe depression in elderly patients — particularly with cardiovascular comorbidity that limits pharmacologic options — ECT is often the safest effective treatment available.
Pregnancy
ECT is safe throughout pregnancy and is sometimes preferred over pharmacologic treatment to avoid fetal medication exposure. Practical considerations: obstetric consultation per gestational age, left lateral uterine displacement during procedure in the second and third trimesters, anesthetic selection with fetal considerations in mind. No trimester is specifically contraindicated.
Psychotic depression
Remission rates in psychotic depression approach 80%, substantially higher than with pharmacotherapy combinations. ECT should be considered early (often first-line) rather than after multiple medication failures.
Bipolar disorder
Effective for both bipolar depression and mania. Unlike pharmacologic antidepressants, ECT does not typically precipitate mood switching. Monitor lithium levels carefully around the ECT course — the combination of high lithium levels with ECT may increase cognitive burden.
Catatonia
First-line for catatonia is high-dose lorazepam. ECT is indicated for:
- Benzodiazepine-refractory catatonia (typically after 2–5 days of adequate trial)
- Malignant catatonia with autonomic instability or hyperthermia
- Neuroleptic malignant syndrome unresponsive to supportive management
Response is often dramatic, with substantial improvement possible within 1–3 treatments.
Medical comorbidities
- Cardiovascular disease: Not an absolute contraindication. Most patients can be safely treated with appropriate anesthetic management and pre-treatment (beta-blockade where indicated). Recent MI (typically <3 months) is the highest concern.
- Parkinson's disease: ECT improves both mood and motor symptoms in PD; motor effects are transient but often meaningful.
- Epilepsy: Not a contraindication. Anticonvulsant-related elevated seizure threshold may require higher stimulus dose or brief medication holds.
- Dementia: Not a contraindication, but requires baseline neuropsychological assessment and conservative dosing choices.
- Intracranial lesions: Small, stable lesions without mass effect are typically not contraindications. Unstable aneurysms, recent hemorrhage, or lesions with meaningful mass effect warrant deferral and neurosurgical consultation.
Referring a patient
How ECT referrals flow through the Prisma Health Neuromodulation Program.
Referral pathway
- Initial referral call or faxed referral form to the Neuromodulation Program at the Behavioral Health and Wellness Pavilion
- Records review by the coordination team; additional records requested as needed
- Outpatient ECT consultation scheduled (typically 1–3 weeks out for non-urgent; expedited for urgent/inpatient referrals)
- Medical clearance and anesthesia evaluation scheduled
- Treatment course scheduled at the appropriate facility — inpatient at Greenville Memorial Hospital; outpatient at Baptist Hospital Columbia or Baptist Easley Hospital depending on geography and clinical factors
What to include in a referral
- Demographics and contact information
- Primary diagnosis and target symptoms for ECT
- Medication history with doses, durations, and responses (a summary list is fine)
- Psychotherapy history
- Prior neuromodulation (TMS, ketamine, prior ECT) with response
- Medical comorbidities and current medications
- Recent psychiatric evaluation or hospitalization records
- Cognitive concerns or baseline neuropsychological assessment, if available
- Urgency level (active suicidality, inpatient status, catatonia)
Urgent referrals
Flag as urgent:
- Active suicidality with severe depression unresponsive to medications
- Severe inanition or catatonia
- Severe psychotic depression
- Currently inpatient requiring rapid definitive treatment
- Pregnancy with severe psychiatric illness where medications are contraindicated
- Neuroleptic malignant syndrome unresponsive to supportive care
Prisma Health Neuromodulation Program
For ECT consultations, referrals, and clinical questions:
Behavioral Health and Wellness Pavilion
725 Grove Road, Greenville, SC 29605
Evaluations: Grove Road office
Inpatient ECT: Greenville Memorial Hospital
Outpatient ECT: Baptist Hospital Columbia / Baptist Easley Hospital
Adam Hart, MD — Medical Director for ECT Services
Prisma Health Neuromodulation Program
References
Key sources cited throughout this page. Organized thematically rather than in order of appearance.
Efficacy and outcomes
- UK ECT Review Group. Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis. Lancet 2003;361(9360):799–808. PMID: 12642045
- Anderson IM. Electroconvulsive therapy (ECT) versus sham ECT for depression: do study limitations invalidate the evidence (and mean we should stop using ECT)? BJPsych Advances 2021;27(5):285–291.
- Meechan CF, Laws KR, Young AH, McLoughlin DM, Jauhar S. A critique of narrative reviews of the evidence-base for ECT in depression. Epidemiol Psychiatr Sci 2022;31:e10.
- Espinoza RT, Kellner CH. Electroconvulsive Therapy. N Engl J Med 2022;386(7):667–672. PMID: 35172057
- Belge JB, van Eijndhoven P, Mulders PCR. Mechanism of action of ECT in depression. Curr Top Behav Neurosci 2024;66:279–295. PMID: 37962811
- Semple DM, Suveges S, Steele JD. Electroconvulsive therapy response and remission in moderate to severe depressive illness: a decade of national Scottish data. Br J Psychiatry 2024;225(6):547–555.
- Petrides G, Fink M, Husain MM, et al. ECT remission rates in psychotic versus nonpsychotic depressed patients: a report from CORE. J ECT 2001;17(4):244–253. PMID: 11731725
- Prudic J, Olfson M, Marcus SC, Fuller RB, Sackeim HA. DSM melancholic features are unreliable predictors of ECT response: a CORE publication. J ECT 2007;23(3):181–186. PMID: 17804986
- Keller JJ, Evans DL, Amlee J, Achtyes ED. Depression remission and response rates and anxiety response as a predictor of depression response in a community electroconvulsive therapy clinic. Prim Care Companion CNS Disord 2025;27(4):25m03939. PMID: 40875885
- Dunne RA, Cannon C, Mayer C, et al. Ultrabrief pulse electroconvulsive therapy for depression: a systematic review and meta-analysis. Mol Psychiatry 2025 (published online November 2025).
Electrode placement and dosing
- Sackeim HA, Decina P, Kanzler M, Kerr B, Malitz S. Effects of electrode placement on the efficacy of titrated, low-dose ECT. Am J Psychiatry 1987;144(11):1449–1455. PMID: 3314538
- Sackeim HA, Prudic J, Devanand DP, et al. Effects of stimulus intensity and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. N Engl J Med 1993;328(12):839–846. PMID: 8441428
- Sackeim HA, Prudic J, Devanand DP, et al. A prospective, randomized, double-blind comparison of bilateral and right unilateral electroconvulsive therapy at different stimulus intensities. Arch Gen Psychiatry 2000;57(5):425–434. PMID: 10807482
- McCall WV, Reboussin DM, Weiner RD, Sackeim HA. Titrated moderately suprathreshold vs fixed high-dose right unilateral electroconvulsive therapy. Arch Gen Psychiatry 2000;57(5):438–444. PMID: 10807483
- Sackeim HA, Prudic J, Nobler MS, et al. Effects of pulse width and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. Brain Stimul 2008;1(2):71–83. PMID: 19756236
- Kolshus E, Jelovac A, McLoughlin DM. Bitemporal v. high-dose right unilateral electroconvulsive therapy for depression: a systematic review and meta-analysis of randomized controlled trials. Psychol Med 2017;47(3):518–530. PMID: 27780482
- Pisvejc J, Hyrman V, Sikora J, et al. A comparison of brief and ultrabrief pulse stimuli in unilateral ECT. J ECT 1998;14(2):68–75.
- Kho KH, van Vreeswijk MF, Simpson S, Zwinderman AH. A meta-analysis of electroconvulsive therapy efficacy in depression. J ECT 2003;19(3):139–147.
Mechanism of action
- Brunoni AR, Baeken C, Machado-Vieira R, et al. BDNF blood levels after electroconvulsive therapy in patients with mood disorders: a systematic review and meta-analysis. World J Biol Psychiatry 2014;15(5):411–418.
- Haskett RF. Electroconvulsive therapy's mechanism of action: neuroendocrine hypotheses. J ECT 2014;30(2):107–110.
- Beall EB, Malone DA, Dale RM, et al. Effects of electroconvulsive therapy on brain functional activation and connectivity in depression. J ECT 2012;28(4):234–241.
- Esel E, Kose K, Hacimusalar Y, et al. The effects of electroconvulsive therapy on GABAergic function in major depressive patients. J ECT 2008;24(3):224–228.
- Minelli A, Zanardini R, Abate M, Bortolomasi M, Gennarelli M, Bocchio-Chiavetto L. Vascular Endothelial Growth Factor (VEGF) serum concentration during electroconvulsive therapy (ECT) in treatment resistant depressed patients. Prog Neuropsychopharmacol Biol Psychiatry 2011;35(5):1322–1325.
- Dyrvig M, Christiansen SH, Woldbye DP, Lichota J. Temporal gene expression profile after acute electroconvulsive stimulation in the rat. Gene 2014;539(1):8–14.
- Perrin JS, Merz S, Bennett DM, et al. Electroconvulsive therapy reduces frontal cortical connectivity in severe depressive disorder. Proc Natl Acad Sci USA 2012;109(14):5464–5468.
- Mulders PC, van Eijndhoven PF, Pluijmen J, Schene AH, Tendolkar I, Beckmann CF. Default mode network coherence in treatment-resistant major depressive disorder during electroconvulsive therapy. J Affect Disord 2016;205:130–137.
- Singh A, Kar SK. How Electroconvulsive Therapy Works? Understanding the Neurobiological Mechanisms. Clin Psychopharmacol Neurosci 2017;15(3):210–221.
Cognitive effects and safety
- Semkovska M, McLoughlin DM. Objective cognitive performance associated with electroconvulsive therapy for depression: a systematic review and meta-analysis. Biol Psychiatry 2010;68(6):568–577. PMID: 20673880
- Watts BV, Groft A, Bagian JP, Mills PD. An examination of mortality and other adverse events related to electroconvulsive therapy using a national adverse event report system. J ECT 2011;27(2):105–108. PMID: 20966769
- Tørring N, Sanghani SN, Petrides G, Kellner CH, Ostergaard SD. The mortality rate of electroconvulsive therapy: a systematic review and pooled analysis. Acta Psychiatr Scand 2017;135(5):388–397.
Suicide and mortality
- Odermatt J, Sarlon J, Schaefer N, et al. Electroconvulsive therapy reduces suicidality and all-cause mortality in refractory depression: a systematic review and meta-analysis of neurostimulation studies. Neurosci Appl 2025;4:105520. PMID: 41323432
- Rhee TG, Shim S, Nasir M, et al. Longitudinal associations of electroconvulsive therapy with all-cause mortality and suicide deaths in severe unipolar or bipolar depression: a systematic review and meta-analysis. BMJ Ment Health 2025;28(1):e302083.
- Kaster TS, Blumberger DM, Gomes T, Sutradhar R, Wijeysundera DN, Vigod SN. Risk of suicide death following electroconvulsive therapy treatment for depression: a propensity score-weighted, retrospective cohort study in Canada. Lancet Psychiatry 2022;9(6):435–446.
Continuation treatment
- Sackeim HA, Haskett RF, Mulsant BH, et al. Continuation pharmacotherapy in the prevention of relapse following electroconvulsive therapy: a randomized controlled trial. JAMA 2001;285(10):1299–1307. PMID: 11255384
- Kellner CH, Knapp RG, Petrides G, et al. Continuation electroconvulsive therapy vs pharmacotherapy for relapse prevention in major depression: a multisite study from CORE. Arch Gen Psychiatry 2006;63(12):1337–1344.
ECT vs. alternatives
- Berlim MT, Van den Eynde F, Daskalakis ZJ. Efficacy and acceptability of high frequency repetitive transcranial magnetic stimulation (rTMS) versus electroconvulsive therapy (ECT) for major depression: a systematic review and meta-analysis of randomized trials. Depress Anxiety 2013;30(7):614–623. PMID: 23349112
- Ren J, Li H, Palaniyappan L, et al. Repetitive transcranial magnetic stimulation versus electroconvulsive therapy for major depression: a systematic review and meta-analysis. Prog Neuropsychopharmacol Biol Psychiatry 2014;51:181–189. PMID: 24556538
- Anand A, Mathew SJ, Sanacora G, et al. Ketamine versus ECT for Nonpsychotic Treatment-Resistant Major Depression (ELEKT-D). N Engl J Med 2023;388(25):2315–2325. PMID: 37224232
- Rhee TG, Shim SR, Forester BP, et al. Efficacy and Safety of Ketamine vs Electroconvulsive Therapy Among Patients With Major Depressive Episode: A Systematic Review and Meta-analysis. JAMA Psychiatry 2022;79(12):1162–1172. PMID: 36260324
- Ekstrand J, Fattah C, Persson M, et al. Racemic Ketamine as an Alternative to Electroconvulsive Therapy for Unipolar Depression: A Randomized, Open-Label, Non-Inferiority Trial (KetECT). Int J Neuropsychopharmacol 2022;25(5):339–349. PMID: 35020871
- Deng ZD, Luber B, McClintock SM, et al. Clinical outcomes of magnetic seizure therapy vs electroconvulsive therapy for major depressive episode: a randomized clinical trial. JAMA Psychiatry 2024;81(3):240–249. (pilot data, n=73)
- Blumberger DM, Mulsant BH, Throop A, et al. Confirmatory efficacy and safety trial of magnetic seizure therapy versus right unilateral ultra-brief electroconvulsive therapy in depression (CREST-MST): a randomised, double-blind, non-inferiority trial in Canada and the USA. Lancet Psychiatry 2026.
Physics and neurophysiology
- Peterchev AV, Rosa MA, Deng ZD, Prudic J, Lisanby SH. Electroconvulsive therapy stimulus parameters: rethinking dosage. J ECT 2010;26(3):159–174. PMID: 20805726
- Ranck JB Jr. Which elements are excited in electrical stimulation of mammalian central nervous system: a review. Brain Res 1975;98(3):417–440.
- Weiner RD, Rogers HJ, Davidson JR, Squire LR. Effects of stimulus parameters on cognitive side effects. Ann N Y Acad Sci 1986;462:315–325.
- Sobin C, Sackeim HA, Prudic J, Devanand DP, Moody BJ, McElhiney MC. Predictors of retrograde amnesia following ECT. Am J Psychiatry 1995;152(7):995–1001. PMID: 7793470
Who responds to ECT — and can we tell before starting?
ECT has the highest response rate of any antidepressant treatment, yet roughly 20–40% of patients will not remit with a standard index course. Predicting individual response has become one of the most active areas of ECT biomarker research — and ECT, uniquely, is the first depression treatment for which imaging biomarkers have crossed the APA's 80% threshold for clinical utility.
Three reasons patients don't respond
Non-response to ECT, like non-response to any psychiatric intervention, usually resolves into one of three categories. Naming the category matters because the next move differs substantially across them.
What clinical variables actually predict response
Two meta-analyses — Haq 2015 (32 studies) and van Diermen 2018 (34 studies) — have characterized which patient features carry real predictive weight and which, despite common belief, do not.
| Predictor | Direction & strength | Source |
|---|---|---|
| Shorter episode duration | Robust predictor of better response. Mean duration in responders ~6.6 months vs. ~14 months in non-responders. | Haq 2015; van Diermen 2018 |
| Absence of prior medication resistance | Robust. Response 70% without prior med failure vs. 58% with — a consistent, modest but clinically relevant effect. | Haq 2015 |
| Psychotic features | Weak-to-moderate predictor of higher response and remission. Effect attenuates when confounders are controlled. | van Diermen 2018; Haq 2015 |
| Older age | Weak predictor of higher response. Notable heterogeneity between studies; mediated in part by psychomotor retardation. | Heijnen 2019; Haq 2015 |
| Catatonia | Response rates historically 85–100% in small series; fewer high-quality predictor studies. | Medda 2015; Ghaziuddin 2020 |
| Bipolar vs. unipolar | Not a significant predictor. No meaningful difference in ECT response. | Haq 2015; Dierckx 2012 |
| Sex, age of onset, # prior episodes | Not significant predictors. | Haq 2015 |
The practical implication: episode duration and prior medication failure are the two clinical variables most worth attending to when setting expectations. Features often cited as "classic" indications — bipolarity, number of prior episodes — don't carry the predictive weight they're assumed to.
Biomarker-based prediction: where the field actually stands
Imaging and neurophysiologic biomarkers have moved further for ECT than for any other depression treatment. In 2012 the APA research council proposed 80% sensitivity and specificity as a threshold for clinical biomarker utility. ECT imaging biomarkers have now met that threshold in multicenter work; medication biomarkers have not (Bruin 2024).
Multimodal neuroimaging
Bruin 2024 — GEMRIC multicenterGlobal ECT-MRI Research Collaboration, 189 patients across 7 centers. Multimodal models combining structural and resting-state functional MRI reached ~80% sensitivity and ~83% specificity for remission prediction with external validation — notably higher than unimodal or medication-biomarker models, and the first ECT biomarker to hit the APA threshold in multicenter data.
Structural gray matter
Jiang 2017; Redlich 2016Pre-ECT gray matter density in six regions (right hippocampus/parahippocampus, right orbitofrontal gyrus, ITG, left postcentral/precuneus, SMA, lingual gyrus) predicted remission at 86–90% accuracy across three independent age-matched datasets. Redlich 2016 showed a small degree of preserved subgenual cingulate structure predicts response with ~78% accuracy and 100% sensitivity.
Individual alpha peak frequency
Voetterl 2023 — Nature Mental HealthThe same "Brainmarker-I" that stratifies TMS response also stratifies ECT: the low-iAPF subgroup showed highest remission to ECT, while iAPF ≈ 10 Hz favored 10 Hz left DLPFC rTMS and higher iAPF favored 1 Hz right DLPFC rTMS. Cheap, fast, repeatable; validated across independent cohorts. The most plausible near-term deployable predictor.
sgACC activity & connectivity
Argyelan 2016; Leaver 2018; van Waarde 2015Baseline subgenual cingulate activity and fronto-temporal functional connectivity carry predictive signal for ECT outcome. The sgACC has emerged as a shared node for ECT and rTMS response prediction — different treatments, same circuit relevance — consistent with the broader network model of depression.
What this means for practice today
None of these biomarker tools are yet standard of care, and none should be used to deny ECT to a patient who would otherwise meet criteria. The evidence base for ECT efficacy is strong, the alternatives in severe and urgent depression are limited, and imaging-guided patient selection is not yet deployable outside research settings. What is deployable today:
- Attend to the two robust clinical predictors — episode duration and prior medication resistance — when counseling patients on expected response. These are more informative than features often cited (bipolarity, melancholia).
- Screen and treat medical contributors before — or concurrent with — the index course. Thyroid, sleep apnea, B12/folate, pain, substance use, and emerging neurocognitive disease are the highest- yield targets.
- Assess the psychosocial environment the patient will return to. A robust discharge plan, close continuation-ECT or pharmacologic follow-up, and concrete attention to housing, interpersonal safety, and ongoing stressors predict durability of response more than any stimulation parameter.
- For non-responders, consider whether a partial-response pattern suggests a medical or psychosocial driver rather than a biological ECT-resistance — and whether a pharmacologic augmentation strategy or transition to maintenance ECT, ketamine, or VNS is the right next step, rather than continued index-course extension.
Patients who don't respond to ECT aren't failing the treatment. The treatment is running into something — in the biology, the body, or the environment — that the protocol alone can't reach. The clinician's job is to figure out which, and act on it.
- Haq AU, Sitzmann AF, Goldman ML, Maixner DF, Mickey BJ. Response of depression to electroconvulsive therapy: a meta-analysis of clinical predictors. J Clin Psychiatry. 2015;76(10):1374–1384. doi:10.4088/JCP.14r09528. PMID: 26528644.
- van Diermen L, van den Ameele S, Kamperman AM, et al. Prediction of electroconvulsive therapy response and remission in major depression: meta-analysis. Br J Psychiatry. 2018;212(2):71–80. doi:10.1192/bjp.2017.28. PMID: 29436330.
- Bruin WB, Oltedal L, Bartsch H, et al. Development and validation of a multimodal neuroimaging biomarker for electroconvulsive therapy outcome in depression: a multicenter machine learning analysis. Psychol Med. 2024;54(3):495–506. doi:10.1017/S0033291723002040.
- Jiang R, Abbott CC, Jiang T, et al. SMRI biomarkers predict electroconvulsive treatment outcomes: accuracy with independent data sets. Neuropsychopharmacology. 2018;43(5):1078–1087. doi:10.1038/npp.2017.165. PMID: 28758644.
- Redlich R, Opel N, Grotegerd D, et al. Prediction of individual response to electroconvulsive therapy via machine learning on structural magnetic resonance imaging data. JAMA Psychiatry. 2016;73(6):557–564. doi:10.1001/jamapsychiatry.2016.0316. PMID: 27145449.
- Voetterl HTS, Sack AT, Olbrich S, et al. Alpha peak frequency-based Brainmarker-I as a method to stratify to pharmacotherapy and brain stimulation treatments in depression. Nat Mental Health. 2023;1:1023–1032. doi:10.1038/s44220-023-00160-7.
- Leaver AM, Wade B, Vasavada M, et al. Fronto-temporal connectivity predicts ECT outcome in major depression. Front Psychiatry. 2018;9:92. doi:10.3389/fpsyt.2018.00092.